Pharmacy Benefit Managers (PBMs) have received a lot of negative publicity lately. Here is some more: A new whistleblower lawsuit has opened another door that reveals more skeletons in the PBM’s closet. Does this skeleton make PBMs look like a friend to Pharma?
A former employee of CVS Health, which operates the largest PBM in the country, accuses the company of driving prescriptions for Medicare Part D beneficiaries away from generic drugs. The alleged goal was to increase revenues derived from rebates on brand-name drugs, which represent much higher profits to a PBM than generic drugs. Yes, you read that right. Branded drugs may represent a profit to PBMs. Read on…
The PBM role isn’t supposed to help drug manufacturers
A PBM is paid by its clients to lower the cost of the pharmacy benefit. Whether the client is an insurance company or a self-funded employer, they pay the PBM to control drug costs. This puts the PBM on the opposite side of the negotiating table from drug manufacturers, who want to sell more drugs. Generic drugs should be a PBM’s best friend, not a manufacturer of expensive branded drugs.
How a PBM makes money promoting branded drugs
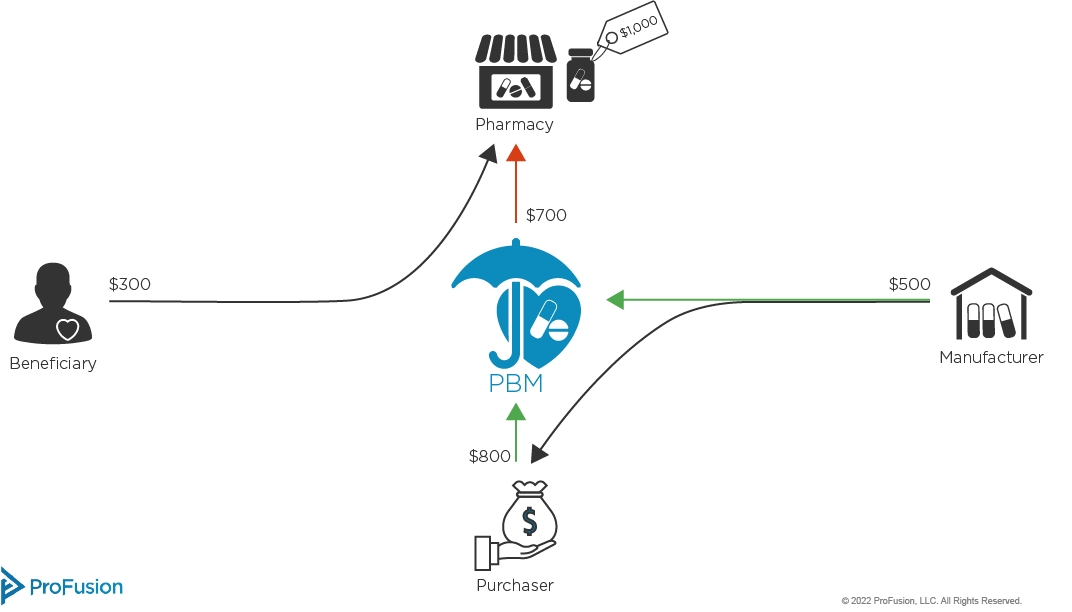
It may seem contradictory that a PBM could make money by filling prescriptions with more expensive drugs. Here is a quick description of how that works (see illustration below):
- Let’s say a branded drug has a list price of $1000. The PBM places it on the highest formulary tier, which requires a 50% coinsurance payment from the patient
- The PBM then reaches an agreement with the drug manufacturer to get a 50% rebate in return for a better formulary tier, one with a 30% coinsurance from the patient
- The patient pays $300 as her share of costs. The manufacturer pays $500 in rebates
- This leaves a gross cost of $200 to the PBM
- The PBM typically recoups some drug costs from its clients (like employers). In a stroke of benevolence, the PBM only charges the employer 80% of list price. This looks like a good discount to the employer, right?
- Here’s the money bullet: In our $1000 example, the PBM has paid $200 for the drug after patient cost sharing and manufacturer discounts, but has collected $800 from its client
- Generic drugs are different in many ways. One, they are less expensive, and any margins from filling that prescription are smaller. In addition, rebates on generics are almost non-existent compared to branded drug rebates
Simplified PBM Contract Example
You may have heard PBMs claim they are now passing 100% of the rebates to their clients. There are accounting tricks that allow the PBM to retain a significant portion of the rebates, which is a good topic to discuss another time. While sharing rebates may lower the profit calculations we just described, it still means there is more profit in drugs that have large rebates.
Who does this calculation affect?
This scheme hurts patients. By blocking access to less expensive generic drugs, a PBM forces many patients to pay higher cost sharing required for brand name drugs. It also increases costs for the Medicare program, as it ultimately pays for drugs under the Part D benefit.
What the suit may tell us about PBMs
PBMs are on the defensive. There are many allegations from powerful stakeholders that, if proven true, may eventually disrupt the PBM business model. In response to these allegations, PBMs have made claims and statements to defend that model. Here are two ways this lawsuit shines a light on the skeletons we mentioned at the beginning:
“PBMs pass all mandated rebates to the payer” – PBMs defend rebates by claiming the money is used to lower monthly premiums. If what this suit alleges is true, then CVS sees rebates as a profit driver for its own bottom line, not as a net cost-saving measure. CVS even admits as much in its Annual Report this year, stating that changes to the rebate laws would “materially” affect the company’s financial results.
- “PBMs save the healthcare system billions of dollars in drug costs through rebates” – Many stakeholders, including the Federal Trade Commission, see drug rebates as a driver of higher drug costs. An analysis by the University of Southern California concludes that for every $1.00 spent on rebates, pharmaceutical manufacturers raise their drug list prices by $1.17. Again, if the actions alleged in the lawsuit are true, then it may be proof the FTC and USC are correct.
Impact on Pharma
This lawsuit alleges manufacturers of branded drugs are gaining market share with the assistance of a PBM (we won’t list the specific pharma companies described in the whistleblower suit, as the legal process is just beginning). But rebates are a standard strategy used by drug manufacturers to gain market share, so this is not a new approach on their part. And if a manufacturer does gain market share this way, it clearly isn’t a gesture of good will from the PBM. In essence, a demand for rebates is a demand for a share in drug profits. A rebate agreement is the way a PBM says “we’ll increase your sales as long as you give us X% of the revenue.”
When viewed in that lens, the rebate transaction would seem to run afoul of anti-kickback and other related laws. Are we nearing the end of the drug rebate era, as the FTC and others are considering? It may appear so