New price transparency rules set by the government are an opportunity to save money. Not for hospitals, not for payers, but for you and me. Isn’t that a nice change of pace?
What’s changed?
There are two transparency rules published by the Department of Health and Human Services (HHS). One dictates that hospitals publish what they charge payers, and another that requires payers to publish what they reimburse providers for their services. Both of those rules can save us, the beneficiaries, significant money.
What the data tells us so far
Although many hospitals haven’t complied with this new HHS rule, the data we have seen is staggering. Look at this Los Angeles market analysis as an example:
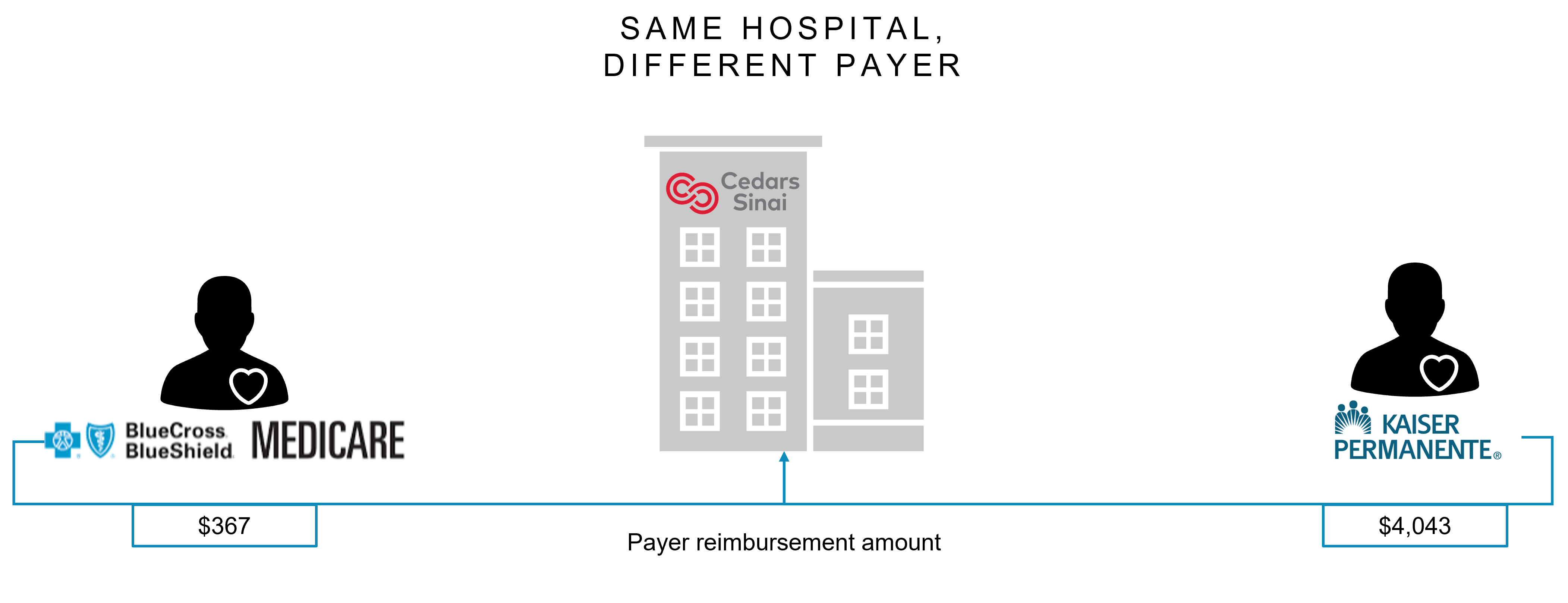
Variance within the same hospital
This scenario looks at how one hospital is paid vastly different amounts:
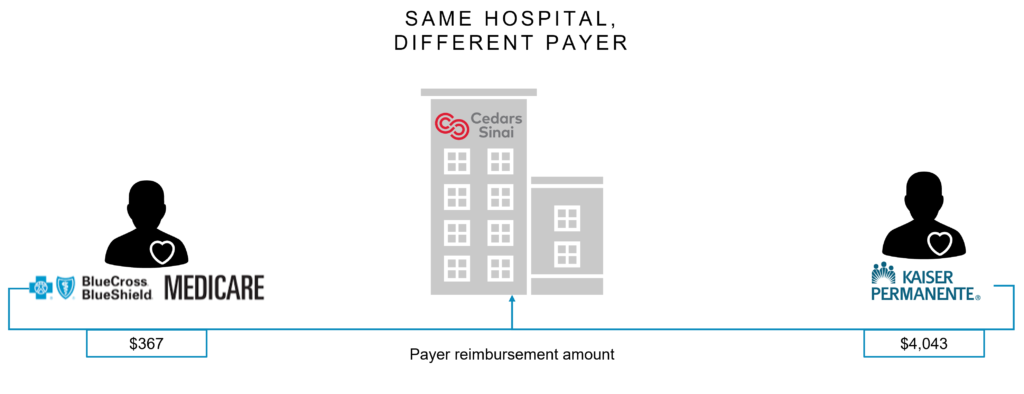
Cedars-Sinai gets reimbursed $367 by BCBS Medicare Advantage for a brain MRI. Kaiser’s commercial plans pay Cedars-Sinai $4,043 for the same procedure
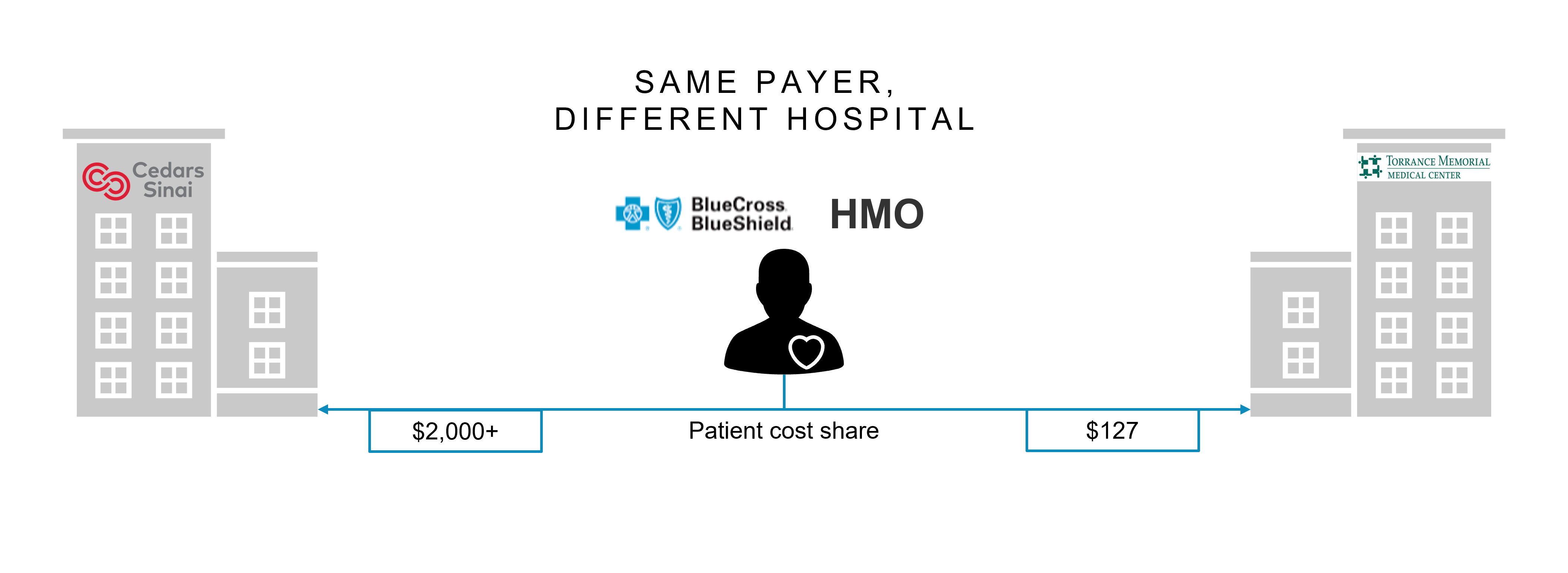
Variance between hospitals
This scenario looks at how a payer allows vastly different amounts to different network providers:
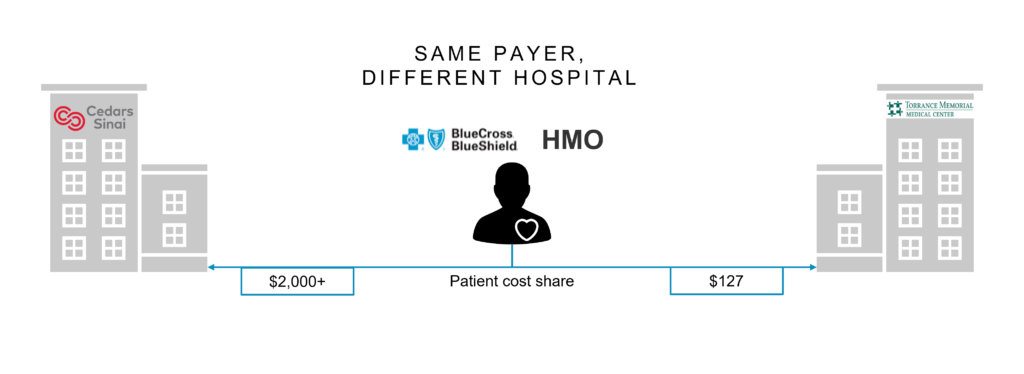
If a patient covered by a BCBS HMO plan walks into Cedars-Sinai for a brain MRI, she will pay over $2,000 as her share of cost (which is based on hospital charges). If she carried her same insurance policy 20 miles down the road to the Torrance Medical hospital, she would only pay $127
This quick look into a small sample of data tells us all we need to know; there are significant differences in costs between hospitals and the contracts they have with payers.
How to use this data
Viewing the data yourself may be time consuming because it isn’t consolidated in one place for a one-stop shopping experience (the government has done exactly this with the Health Insurance Exchanges website). It requires going to a website hosted by the (rare?) hospital actually publishing its data. To share an example of what you may find, here is a link to Banner Health’s site, which captures different charges for its many sites of care.
Payer data sets
As of this past July 1, payers must publish the price (the “allowable” charge) they negotiated for every service with every physician, hospital, nursing home, etc. in their network. That’s a lot. Self-funded employers must do the same thing, as they are considered the “payer” under the HHS rule. As of January 1 of next year, payers must also publish their allowable charges for 500 “shoppable” services, which generally can be scheduled ahead of time. In theory, these data sets will be somewhat redundant.
We save money two ways
These data sets offer us two ways to save money.
The first process is obvious. If you can see the allowable charge for an x-ray, you can check the local hospital, the local imaging center, and a local doctor’s office to see what your insurer has negotiated. If you have to pay a coinsurance (say, 20%) for the service, you’ll save money by going to the cheapest site of care.
The second opportunity to save is higher up the purchasing chain. If you get your insurance from your employer (as the majority of Americans do), they can leverage this data in their own negotiations with providers. Employers can shop around for the best prices, just like you.
And they need to. A Rand Corporation study revealed that payers and employers pay an average of 224% of what Medicare pays.
In fact, employers are required to negotiate the lowest price they possibly can. Because the money to pay for healthcare comes from wages and benefits, they have a fiduciary responsibility to make decisions based solely in the interests of participants in the health plan. Purchasing decisions cannot be made with company profit in mind. This means leveraging access to pricing can lead to lower costs that should be transferred to you, the beneficiary.
How these rules impact Pharma
Many aspects of drug costs and net pricing are still shrouded behind the curtain. The HHS transparency rules don’t reveal all price points for a drug (like 340B) or rebates from manufacturers. This mitigates the impact on Pharma.
For medical benefit drugs, the hospital data set is required to show what they charge for various J-codes. The prices of pharmacy benefit drugs are not included in either the hospital or payer data sets. This may be due to the fact that pharmacies (and PBMs) are more directly involved in negotiating those drugs than other stakeholders.
One possible take-away from all this data is the insight it provides on the disparity between what a hospital may pay for an injectable/infusible drug versus what it charges for it. With so much controversy surrounding drug costs in our country, seeing the mark-up hospitals charge and how that may impact a patient’s share of cost is quite revealing. Maybe this will divert some of the spotlight away from manufacturers on the topic.